GLP-1 / GIP Dual Agonists
A new generation of obesity and diabetes drugs that work two hormone pathways at once.
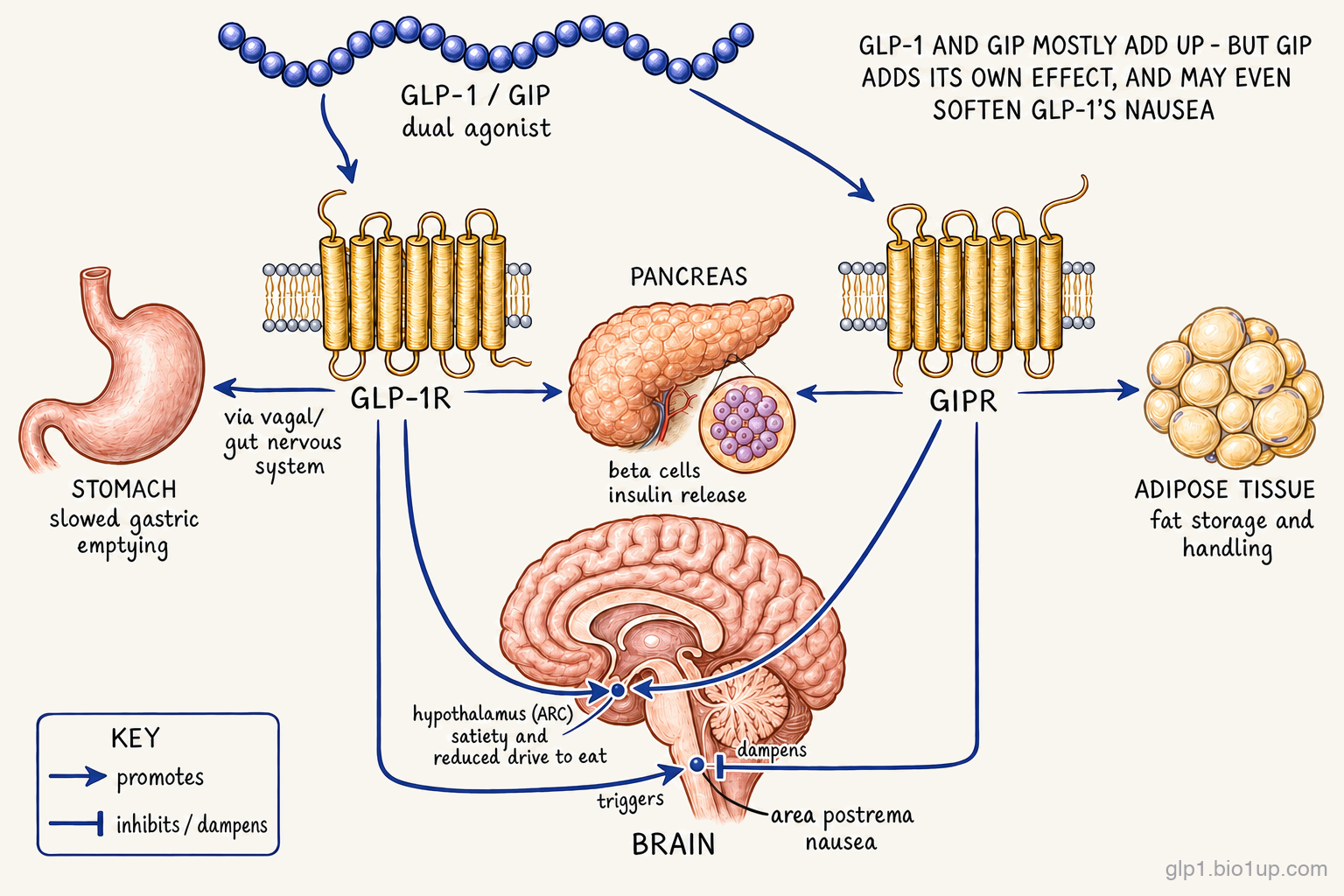
GLP-1 brakes hunger; GIP amplifies the insulin response and may dampen nausea. Dual agonists combine these effects. The result has reset how much weight a single drug can take off.
Counts reflect publicly disclosed programs in our database. Earlier-stage or undisclosed assets may not yet be represented.
Re-checked August 3, 2026
Every claim on this page is re-verified against sources including ClinicalTrials.gov, regulatory actions, press releases, and the published literature, all tracked in the GLP-1 Observer database.
GLP-1 / GIP dual agonists are a class of obesity and diabetes drugs that activate two different hormone receptors with a single molecule. The GLP-1 receptor is the better-known one. It's how GLP-1 mono-agonists like semaglutide (sold as Ozempic for diabetes and Wegovy for obesity) work, in part by reducing appetite and slowing digestion. The GIP receptor is the new addition: it amplifies insulin release when blood sugar rises, and appears to soften the nausea commonly caused by GLP-1-only drugs. The first drug in this class, tirzepatide (sold as Mounjaro for diabetes and Zepbound for weight loss), reached the U.S. market in 2022 and quickly became the most effective weight-loss drug ever brought to market. Several newer dual agonists are now in late-stage trials, racing to match or exceed it.
How dual agonists work
The basic insight is that GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) don't do the same job. They complement each other.
Both hormones are called incretins: after a meal, both signal the pancreas to release insulin in proportion to how much glucose just hit the bloodstream. That shared insulin role is the historical reason this whole drug class exists. What sets the two hormones apart is what each does beyond insulin.
Beyond insulin, GLP-1 acts strongly on appetite and digestion. It's one of the signals that tells the brain you're full, slows the rate at which food leaves the stomach, and suppresses the hormone glucagon at the pancreas. Drugs in the GLP-1 family (semaglutide, sold as Ozempic and Wegovy, and the rest) copy that signal at much higher levels than the body produces on its own, and that's how they reduce hunger and produce weight loss.
GIP is the other half of the incretin story. Its action on the pancreas is, by some measures, more powerful than GLP-1's: GIP is responsible for a larger share of the meal-stimulated insulin response in healthy physiology. GIP receptors are also expressed in the brain, with hypothalamic receptors implicated in appetite regulation and brainstem receptors increasingly thought to soften nausea. This central action may be part of why dual agonists produce larger weight loss than GLP-1 drugs alone, though the brain side of the GIP story is still being worked out. GIP also influences how adipose tissue stores and metabolizes fat. Until tirzepatide, no approved drug had targeted GIP at all.
A dual agonist activates both receptors at once with a single molecule. That sounds like a small change, but it produces effects neither pathway can deliver alone. In tirzepatide's pivotal weight-loss trial, patients on average lost about 22% of their body weight at the highest dose among those who stayed on the drug, roughly a third more than semaglutide (Wegovy) achieved in its own pivotal trial, a gap that semaglutide's newer high-dose version has since narrowed. Patients also reported better tolerability than what you'd expect from doubling up on receptor activation, which is part of why the GIP component is still being studied for its possible role in softening side effects.
Not every dual-targeting drug is built the same way. Some dual agonists lean more on GLP-1, some more on GIP, and at least one notable related program (MariTide from Amgen) takes the opposite bet on GIP by blocking the receptor instead of activating it. Those variations are covered below in Related and adjacent mechanisms.
The competitive landscape
Landscape as of July 2026Tirzepatide stands alone on the U.S. and European market today, and that's not likely to change there for at least another year. China is moving faster: Hengrui's HRS9531 was accepted for obesity review by China's drug regulator in September 2025 and is still pending there. The chasing pack of dual agonists that could be the next approved options is in late-stage trials, and the makeup of that group is one of the more interesting stories in obesity drug development right now.
Viking Therapeutics is the lead Western challenger, with VK2735 now in two large Phase 3 trials: VANQUISH 1 (4,500 patients) in obesity and VANQUISH 2 (1,100 patients) in obesity plus type 2 diabetes. Viking is also developing an oral version of VK2735, a separate bet on whether dual-agonist efficacy can survive the transition from injection to pill. Roche is the other Western contender: its enicepatide (CT-388) entered two Phase 3 obesity trials in 2026, a step behind Viking on timing.
The other Phase 3 contenders are mostly Chinese. Hengrui's HRS9531 is the furthest along, with a Phase 3 obesity trial already completed (showing up to 19.2% weight loss over 48 weeks), its head-to-head trials against semaglutide in obesity underway, and a 9,262-patient cardiovascular outcomes trial now recruiting, the first China-origin dual agonist to take on that hardest endpoint. BrightGene's BGM0504, Hansoh's HS-20094, and several others are running large Phase 3 trials in diabetes. Kailera Therapeutics, a newly Nasdaq-listed company that licensed Hengrui's obesity pipeline for markets outside China, is running a particularly large Phase 3 program (more than 4,000 patients across three trials) for KAI-9531, which is the same molecule as HRS9531 under a different name. The pace at which Chinese-origin assets have reached late-stage testing has been one of the genuine surprises of the past two years.
The race to watch over the next 12 to 18 months: whether VK2735 or any of the Chinese contenders actually match tirzepatide's roughly 22% weight loss, and whether any improve on tolerability as well as efficacy.
Drugs in this class
| Drug | Developer | Formulation | Stage | Conditions |
|---|---|---|---|---|
| Tirzepatide | Eli Lilly | Weekly injection | Approved | Type 2 diabetes, obesity |
| VK2735 | Viking Therapeutics | Weekly injection (oral version in earlier trials) | Phase 3 | Obesity, type 2 diabetes |
| HRS9531 / KAI-9531 | Hengrui / Kailera Therapeutics | Weekly injection | Phase 3 | Obesity, type 2 diabetes, sleep apnea |
| CT-388 (enicepatide) | Roche | Weekly injection | Phase 3 | Obesity, type 2 diabetes |
Also in this class
- BGM0504 · BrightGene · Phase 3 (type 2 diabetes)
- HS-20094 · Hansoh Pharmaceutical · Phase 3 (type 2 diabetes)
- HDM1005 · Huadong Pharmaceutical · Phase 3 (type 2 diabetes)
- RAY1225 · Raynovent · Phase 3 (type 2 diabetes)
- CT-868 · Roche (Carmot Therapeutics) · Phase 2
- NNC0519-0130 · Novo Nordisk · Phase 2
- LY3493269 · Eli Lilly · Phase 1
Brenipatide (Eli Lilly's LY-3537031), a same-mechanism dual agonist, is in Phase 3 but for non-metabolic indications such as alcohol use disorder and bipolar disorder rather than obesity. Other earlier-stage assets, such as SYH2082, are also in development.
Related and adjacent mechanisms
A few related drug classes don't quite fit the GLP-1 / GIP dual-agonist definition but sit close enough to be worth knowing about, especially if you're trying to understand where the field might be heading.
Activate GLP-1, block GIP: MariTide
Amgen's MariTide (maridebart cafraglutide) does something that initially sounds contradictory to everything above. It still activates the GLP-1 receptor (that part it shares with the dual agonists), but it blocks the GIP receptor instead of activating it. Both approaches have shown weight loss in trials, which seems puzzling: how can opposite actions on the same receptor both produce weight loss? The honest answer is that researchers are still figuring this out. One leading hypothesis is that chronic GIP receptor activation eventually causes the receptor to become desensitized, so a sustained agonist may, over time, functionally resemble a blocker. A competing hypothesis is that agonists and antagonists act on distinct neural populations and pathways. Amgen, for its part, points to human genetic data showing that variants that reduce GIP receptor function are associated with lower body weight. Whatever the resolution turns out to be, both "activate GIP" and "block GIP" are live bets in late-stage testing. MariTide is currently in Phase 3 obesity trials.
Add a third receptor: triple agonists
Eli Lilly's retatrutide adds glucagon receptor activation on top of GLP-1 and GIP. Glucagon raises blood sugar in normal physiology, so adding it to a weight-loss drug initially seems counterproductive. But at pharmacological doses, it also raises energy expenditure: the body burns more calories at rest. Retatrutide has shown the largest weight loss of any drug to date. Its first Phase 3 obesity trial (TRIUMPH-1) reported about 28% weight loss at the top dose in May 2026, well above tirzepatide's roughly 22%, and the rest of its Phase 3 program is still reading out.
Swap GIP for amylin: GLP-1 + amylin combinations
Instead of pairing GLP-1 with GIP, Novo Nordisk has pursued GLP-1 + amylin combinations. Amylin is a separate satiety hormone (released from the pancreas alongside insulin) that suppresses appetite through different brain pathways than GLP-1. CagriSema, a fixed-dose combination of semaglutide (GLP-1) and cagrilintide (amylin), and amycretin, a single molecule that activates both receptors, are both in late-stage testing.
For how tirzepatide stacks up beyond the mechanism, the GLP-1 Verdict grades it on efficacy and tolerability: see its Verdict page.
Frequently asked questions
What is a GLP-1 / GIP dual agonist?
A GLP-1 / GIP dual agonist is a single drug molecule that activates two different gut hormone receptors at once: the GLP-1 receptor (the same target as Ozempic and Wegovy) and the GIP receptor. Both hormones are incretins, meaning both stimulate the pancreas to release insulin after meals. The GLP-1 part also reduces appetite and slows digestion; the GIP part may also act on the brain to help reduce side effects like nausea. The first dual agonist, tirzepatide, was approved in 2022 for type 2 diabetes and 2023 for obesity, and it is the most effective weight-loss drug brought to market so far.
What's the difference between tirzepatide and semaglutide?
Both are gut-hormone drugs used for type 2 diabetes and obesity, but they activate different receptors. Semaglutide (Ozempic, Wegovy) activates only the GLP-1 receptor. Tirzepatide (Mounjaro, Zepbound) activates both the GLP-1 receptor and the GIP receptor with a single molecule. Tirzepatide has produced larger weight loss and lower blood sugar than semaglutide in trials. Patients on tirzepatide's highest dose lost about 22% of body weight on average, compared to about 17% for semaglutide at the standard 2.4 mg Wegovy dose. (Novo's newer high-dose 7.2 mg semaglutide, approved in 2026, reaches about 21% and narrows that gap.) A direct head-to-head obesity trial confirmed tirzepatide's larger effect. All figures here are efficacy estimates - weight loss in patients who stay on the drug; real-world numbers run a few percentage points lower.
Why combine GLP-1 and GIP in one drug?
Because the two pathways share an insulin-release role and add different complementary jobs on top. GLP-1 leans heavily on appetite suppression and slowing digestion. GIP amplifies the insulin response further and appears to influence how the body stores and burns fat. Combining both into a single weekly injection lets one drug hit both pathways at matched doses, which is hard to replicate with two separate drugs. In trials, dual agonists have produced larger weight loss and better blood sugar control than GLP-1 drugs alone.
Are GLP-1 / GIP dual agonists safer than GLP-1 drugs alone?
Side effects are broadly similar: nausea, vomiting, diarrhea, and constipation are the most common with both classes, especially during dose escalation. Some early data suggests dual agonists may produce somewhat less nausea than GLP-1 drugs at comparable weight-loss levels, possibly due to the GIP component, but this is still an active area of study. Like GLP-1 drugs, dual agonists carry warnings about pancreatitis and a rare risk of medullary thyroid cancer (based on rodent studies; the human relevance is debated).
When will the next dual agonist be approved?
Probably not for at least another year in the U.S. or Europe. Several dual agonists are in late-stage trials chasing tirzepatide. None have been submitted for approval in the U.S. or Europe yet, but China's drug regulator accepted Hengrui's obesity filing for HRS9531 in September 2025 and is still reviewing it, so the first non-tirzepatide approval may come there first. The most advanced Western challenger is VK2735 from Viking Therapeutics, in Phase 3 obesity trials. Multiple Chinese-developed assets are also in Phase 3, with Hengrui's HRS9531 the furthest along. The big questions for the next 12 to 18 months: whether any of these match tirzepatide's roughly 22% weight loss, and whether the oral versions in earlier-stage testing can deliver injection-like efficacy.
Recent newsletter coverage
Past pieces from the GLP-1 Observer newsletter that touched on this class.
- June 5, 2026 · Trial Spotlight: China's GLP-1/GIP Dual Goes for the Hardest Endpoint: Hengrui's HRS9531 (ribupatide) begins a 9,262-patient cardiovascular outcomes trial, the first China-origin GLP-1/GIP dual to take on the MACE endpoint against the Western incumbents.
- June 5, 2026 · Mechanism Explained: From Fast-Follower to Licensing Engine: how China became a primary source of licensed obesity assets, with the GLP-1/GIP dual ribupatide as the template for the multi-billion-dollar NewCo deal structure.
- May 15, 2026 · Trial Spotlight: Less Drug, Still Drug - Lilly's Two Maintenance Trials: SURMOUNT-MAINTAIN shows stepping tirzepatide (Zepbound) down to a low dose holds most of the weight off, while stopping outright does not.
References
- Drucker DJ. GLP-1-based therapies for diabetes, obesity and beyond. Nature Reviews Drug Discovery. 2025.
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity. New England Journal of Medicine. 2022. (SURMOUNT-1 pivotal obesity trial)
- Aronne LJ, et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity. New England Journal of Medicine. 2025. (SURMOUNT-5 head-to-head)
- Samms RJ, et al. How May GIP Enhance the Therapeutic Efficacy of GLP-1? Trends in Endocrinology & Metabolism. 2020.
- Willard FS, et al. Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist. JCI Insight. 2020.
Track this class
GLP-1 Observer tracks clinical trials, news, and regulatory milestones across the GLP-1 and obesity-drug landscape, updated daily. See trial timelines, date-change alerts, and weekly roll-ups.