GLP-1 / GIP / Glucagon Triple Agonists
A new generation of obesity and diabetes drugs that activate three hormone pathways at once.
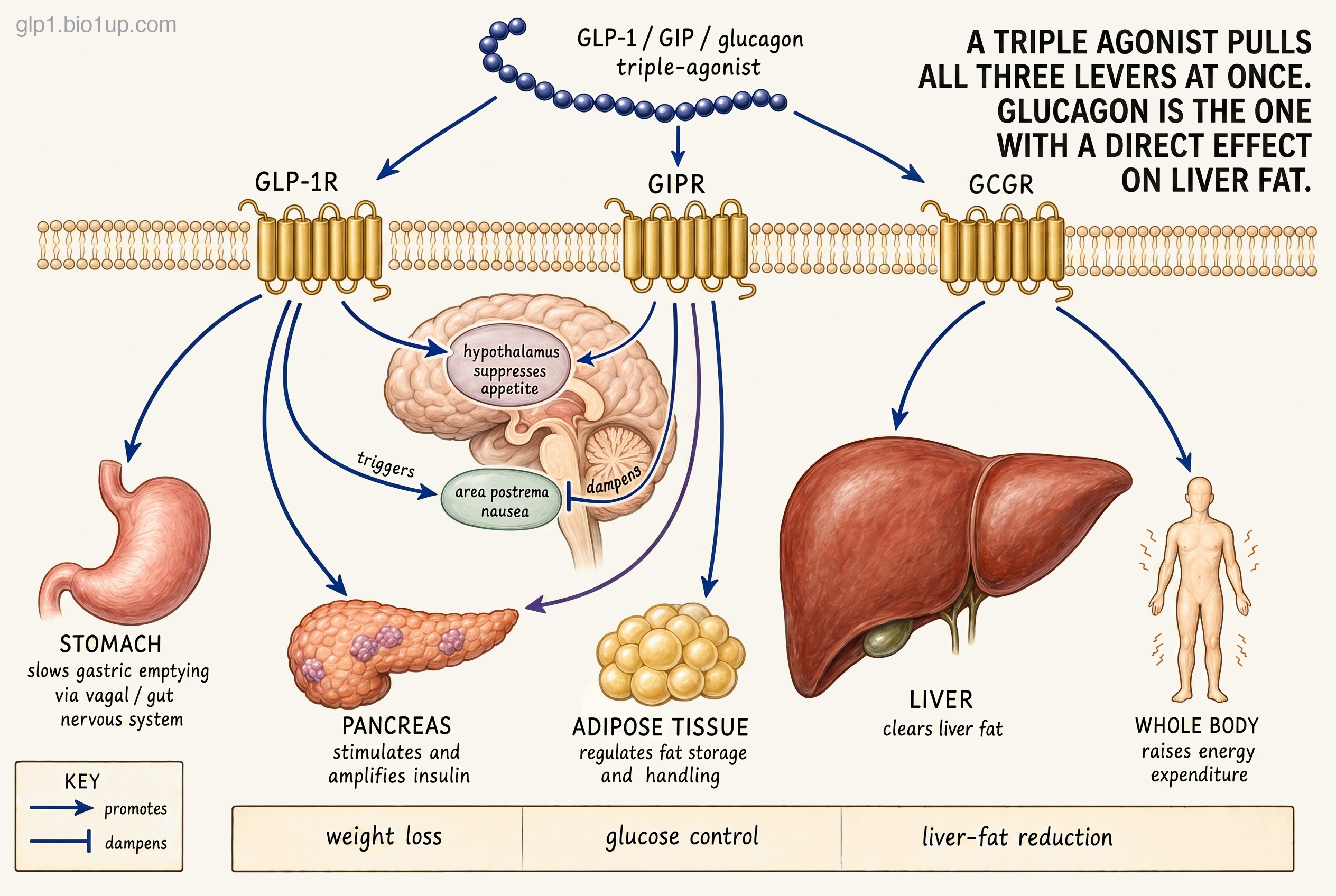
GLP-1 suppresses appetite. GIP amplifies the insulin response and may dampen nausea. Glucagon tells the body to burn more of what's already stored. A triple agonist combines these effects in a single molecule.
Counts reflect publicly disclosed programs in our database. Earlier-stage or undisclosed assets may not yet be represented. No triple agonists are approved as of July 2026. Retatrutide (Eli Lilly) is in global Phase 3; UBT251's China lead (United Laboratories) has entered Phase 3, while Novo Nordisk's program for it outside Greater China now runs Phase 2 trials in both obesity and type 2 diabetes.
Re-checked August 3, 2026
Every claim on this page is re-verified against sources including ClinicalTrials.gov, regulatory actions, press releases, and the published literature, all tracked in the GLP-1 Observer database.
GLP-1 / GIP / glucagon triple agonists are a class of obesity and diabetes drugs that activate three different hormone receptors with a single molecule. GLP-1 reduces appetite, GIP amplifies the insulin response and may dampen nausea, and glucagon prompts the body to burn stored fat, including fat in the liver. Eli Lilly's retatrutide is the lead drug in the class and the first to produce Phase 3 data. Its flagship Phase 3 obesity trial, TRIUMPH-1, read out in May 2026 with an average 28.3% weight loss at the top dose, the largest any obesity drug has shown in a pivotal trial to date. Across its Phase 3 program, retatrutide also surfaced a side effect that Phase 2 had not shown: dysesthesia, a persistent unusual skin sensation. Several other triples are in earlier development, but the class's direction over the next year largely turns on the remaining retatrutide Phase 3 readouts.
How triple agonists work
The core idea is that GLP-1 (glucagon-like peptide-1), GIP (glucose-dependent insulinotropic polypeptide), and glucagon each have their own distinct effects, with some overlap, and stacking all three in one molecule presses more levers than mono-agonists or dual agonists can.
GLP-1 and GIP are both incretins. After a meal, both signal the pancreas to release insulin in proportion to how much glucose just hit the bloodstream. What sets the two hormones apart is what each does beyond insulin.
Beyond insulin, GLP-1 acts strongly on appetite and digestion. It's one of the signals that tells the brain you're full and slows the rate at which food leaves the stomach. Drugs in the GLP-1 family (Ozempic, Wegovy, and the rest) activate that signal more strongly than the body does on its own, and that is how they reduce hunger and produce weight loss.
Beyond insulin, GIP makes several other contributions. Brainstem GIP receptors are increasingly thought to soften the nausea that comes with GLP-1 drugs, and hypothalamic GIP receptors contribute to appetite regulation alongside GLP-1. GIP also influences how adipose tissue stores and metabolizes fat. Tirzepatide (sold as Mounjaro for diabetes and Zepbound for weight loss), the first approved dual agonist, pairs GLP-1 with GIP. In trials, it has produced more weight loss than GLP-1 drugs alone and, so far, has been better tolerated than the scale of that weight loss would predict.
Glucagon is the more counterintuitive addition. In normal physiology, glucagon raises blood sugar. It is the hormone the pancreas releases when blood glucose drops too low, so adding a glucose-raising signal to a diabetes or obesity drug initially sounds like a bad idea. But at the higher doses a drug reaches, glucagon does two metabolically useful things: it acts directly on the liver to drive hepatic fat oxidation, burning the fat stored in liver cells, and it also appears to raise whole-body energy expenditure (the body burns more calories at rest), though how much that resting-burn effect adds to weight loss in humans is still being worked out. Both GLP-1 and GIP stimulate insulin release in parallel, which offsets glucagon's blood-sugar effect, leaving the dramatic reductions in liver fat (and the added calorie burn) that are emerging as a defining feature of the class (retatrutide's Phase 2 liver-fat data is roughly 82% reduction at 24 weeks on the top dose).
A triple agonist activates all three receptors with a single molecule. The open question across the entire class is whether three levers compound each other's effects, or whether the added complexity mostly adds side effects. Retatrutide's Phase 2 data and Phase 3 readouts have begun to answer the first half of that question. Its Phase 3 safety profile has begun to sharpen the second.
The competitive landscape
Landscape as of July 2026Retatrutide is the only triple with Phase 3 results so far, and the data has landed. Its flagship obesity trial, TRIUMPH-1 (about 2,300 adults with obesity or overweight and no type 2 diabetes), read out in May 2026: an average 28.3% weight loss at the top 12 mg dose over 80 weeks, in bariatric-surgery territory and higher than any obesity drug has shown in a pivotal trial to date. The more strategically interesting detail was the dose ladder. A middle 9 mg dose produced 25.9%, and even a low 4 mg dose reached nearly 20% weight loss with a side-effect discontinuation rate that actually fell below placebo, reframing retatrutide from a powerful-but-rough drug into something physicians can titrate from a tolerable floor up to a maximal-loss ceiling. An earlier, smaller Phase 3 trial, TRIUMPH-4 (in patients with obesity and knee osteoarthritis), had reported 28.7% weight loss over 68 weeks in December 2025 along with meaningful knee-pain improvement, and a separate Phase 3 diabetes trial from Lilly's TRANSCEND program reported strong blood-sugar and weight-loss results in March 2026.
The Phase 3 program also surfaced a side effect that had not appeared in Phase 2: dysesthesia, a persistent unusual skin sensation most often described as burning or pins-and-needles. The signal is dose-dependent, and its size has varied across trials: top-dose rates run from about 6 percent in TRIUMPH-3 and about 7 percent in TRIUMPH-2, both reported in July 2026, up to about 21 percent in the smaller TRIUMPH-4 population, with 12.5 percent in the flagship TRIUMPH-1 trial (versus roughly 1 percent or less on placebo). Discontinuation for side-effect reasons at the top dose has ranged from about 8 percent in TRIUMPH-2 up to about 18 percent in the smaller TRIUMPH-4 population (versus roughly 4 to 5 percent on placebo), though Lilly reported that the dysesthesia events themselves were generally mild and rarely the direct cause. The TRIUMPH-1 dose ladder suggests lower doses may preserve most of the weight loss while keeping that signal down, which is exactly what Lilly is now testing.
Behind retatrutide, the clearest credible contender is UBT251, a triple developed by United Laboratories in China and licensed to Novo Nordisk in March 2025 for markets outside Greater China. In a Phase 2 trial in Chinese patients, UBT251 produced 19.7% weight loss at 24 weeks on the top dose, a pace roughly in line with retatrutide's Phase 2 results at the same six-month mark. Novo is now running global Phase 2 trials in both obesity and type 2 diabetes to confirm those results, while United Laboratories has begun Phase 3 testing in China. In parallel, Hanmi (a Korean developer) has two triples in development: efocipegtrutide, in Phase 2 for liver disease, and HM15275, in Phase 2 for obesity. Retatrutide itself has a strong Phase 2 liver-disease result on record (about 82% reduction in liver fat at 24 weeks on the top dose), so the liver-disease question for the class is live across multiple programs.
Beyond these, Novo Nordisk's in-house triple has advanced into Phase 2, and Jiangsu Hengrui's first program (HRS-4729) has also reached Phase 2 in China, though Kailera has yet to start its own trial of the same molecule (KAI-4729) outside China. Eli Lilly's second triple remains in Phase 1. An earlier triple from Sanofi was discontinued in 2019 for portfolio reasons rather than safety.
The race to watch over the next 12 to 18 months: whether retatrutide's remaining Phase 3 readouts, expected later in 2026, confirm the flagship TRIUMPH-1 efficacy without adding new safety signals, whether the lower doses that looked so clean in TRIUMPH-1 hold up at scale, and whether UBT251 delivers when Novo moves it from Chinese testing into a global program.
Drugs in this class
| Drug | Developer | Formulation | Stage | Conditions |
|---|---|---|---|---|
| Retatrutide | Eli Lilly | Weekly injection | Phase 3 | Obesity, type 2 diabetes |
| UBT251 | United Laboratories / Novo Nordisk | Weekly injection | Phase 3 (China) / Phase 2 (global) | Obesity, type 2 diabetes |
| Efocipegtrutide (HM15211) | Hanmi Pharmaceutical | Weekly injection | Phase 2 | Liver disease |
| HM15275 | Hanmi Pharmaceutical | Weekly injection | Phase 2 | Obesity, type 2 diabetes |
| NNC0662-0419 | Novo Nordisk | Weekly injection | Phase 2 | Obesity, type 2 diabetes |
Also in this class
- LY4086940 · Eli Lilly · Phase 1
- HRS-4729 · Jiangsu Hengrui · Phase 2 (China); Kailera plans Phase 1 outside China (as KAI-4729)
Withdrawn and paused
- SAR441255 (Sanofi) was discontinued in 2019 as part of a broader portfolio review, not for safety reasons. The molecule had only reached Phase 1 trials.
Related and adjacent mechanisms
A few related drug classes don't quite fit the triple-agonist definition but sit close enough to be worth knowing about, especially if you're trying to understand where obesity medicine might be heading.
Drop one receptor: the dual agonists
Subtracting any single receptor from a triple produces a class already in late-stage trials. GLP-1 / GIP duals (tirzepatide and its challengers) drop glucagon. GLP-1 / glucagon duals (survodutide, pemvidutide, mazdutide) drop GIP. Both dual classes have shown substantial weight loss, and the GLP-1 / glucagon duals are also showing strong effects on liver fat. Each class carries its own trade-offs: duals are easier to tune than triples (balancing two receptors is simpler than three), while triples bet that the extra lever is worth the added complexity and new tolerability questions.
Pair GLP-1 with amylin: GLP-1 + amylin combinations
Novo Nordisk has pursued a parallel approach that keeps GLP-1 but swaps in amylin, a separate satiety hormone released from the pancreas alongside insulin. Amylin suppresses appetite through different brain pathways than GLP-1. CagriSema (a fixed-dose combination of semaglutide and cagrilintide) and amycretin (a single molecule that activates both receptors) are both in late-stage testing. Others are testing co-administration, pairing a separate amylin analog with an incretin agonist as two injections rather than building one molecule (AstraZeneca's ASCEND program is the clearest example). The GLP-1 + amylin combinations field guide covers them in detail.
Activate GLP-1, block GIP: MariTide
Not every next-generation obesity drug adds more receptor targets. Amgen's MariTide (maridebart cafraglutide) activates GLP-1 but blocks GIP, the opposite of what triples and most duals do. Both approaches have shown weight loss in trials, and researchers are still working out why opposite actions on the same receptor can both produce similar effects. MariTide is currently in Phase 3 obesity trials. Pfizer is testing the same hypothesis through a different architecture: oral co-administration of a GIPR antagonist (PF-07976016, Phase 2) with one of its early-stage oral GLP-1 candidates.
For how retatrutide stacks up beyond the mechanism, the GLP-1 Verdict grades it on efficacy and tolerability: see its Verdict page.
Frequently asked questions
What is a triple agonist?
A triple agonist is a single drug molecule that activates three different hormone receptors at once: GLP-1, GIP, and glucagon. GLP-1 and GIP are both incretins, meaning both stimulate the pancreas to release insulin after meals. The GLP-1 part also reduces appetite and slows digestion; the GIP part may also act on the brain to help reduce side effects like nausea; the glucagon part prompts the body to burn stored fat, including fat in the liver. Eli Lilly's retatrutide is the first triple to reach Phase 3 trials; its flagship Phase 3 obesity trial read out in May 2026 with about 28% average weight loss at the top dose, the largest any obesity drug has shown in a pivotal trial to date, though the Phase 3 program also surfaced a new tolerability signal that Phase 2 had not shown.
How does retatrutide compare to tirzepatide?
Retatrutide has produced larger weight loss than tirzepatide in its own trials, though the two have not been tested head-to-head. In its Phase 2 obesity trial, retatrutide's highest dose produced about 24 percent weight loss over 48 weeks; its flagship Phase 3 obesity trial (TRIUMPH-1) produced about 28 percent over 80 weeks. Tirzepatide (Mounjaro / Zepbound) has produced about 22 percent in its own pivotal obesity trial. These are efficacy estimates (weight loss in patients who stayed on the drug; real-world numbers run a few percentage points lower). Retatrutide's apparent advantage is meaningful, but its Phase 3 data also raised a new side-effect signal that tirzepatide has not shown.
Why add glucagon to a weight-loss drug if it raises blood sugar?
Because at pharmacological doses, glucagon does two useful things: it raises whole-body energy expenditure (the body burns more calories at rest), and it acts directly on the liver to drive hepatic fat oxidation, burning the fat stored in liver cells. Both GLP-1 and GIP stimulate insulin release in parallel, which offsets glucagon's blood-sugar effect. In the triples, this pairing works. Phase 2 and Phase 3 trials of retatrutide showed strong weight loss, and the main metabolic signal went in the opposite direction from what you might expect: better glucose control, with most patients who started with prediabetes returning to normal blood-sugar levels over time. The counterintuitive addition seems to contribute real value to the overall drug effect, with the dramatic effect on liver fat as the clearest attributable benefit.
What are the side effects of triple agonists?
Side effects are broadly similar to GLP-1 and dual agonists: nausea, vomiting, diarrhea, and constipation are most common, especially during dose escalation. Triple agonists add signals from the glucagon component, most notably a dose-dependent heart-rate increase. In retatrutide's Phase 3 trials, a new signal emerged: dysesthesia, a persistent unusual skin sensation often described as burning or pins-and-needles. It is dose-dependent, and its rate has varied across trials: top-dose rates run from about 6 percent in TRIUMPH-3 and about 7 percent in TRIUMPH-2, both reported in July 2026, up to about 21 percent in the smaller TRIUMPH-4 trial, with 12.5 percent in the larger flagship TRIUMPH-1 trial (versus roughly 1 percent or less on placebo). Discontinuation for side-effect reasons at the top dose has ranged from about 8 percent in TRIUMPH-2 up to about 18 percent in TRIUMPH-4, though Lilly reported that the dysesthesia events themselves were generally mild and rarely the direct cause. Whether lower doses can preserve most of the weight loss while reducing the overall side-effect load is an open question.
When will retatrutide be approved?
Most likely 2028, though a decision in late 2027 is possible. In July 2026 Lilly said it plans to submit a Biologics License Application to the FDA in the first quarter of 2027, later than the late-2026 filing it had previously indicated, because it is still completing the manufacturing and quality-control data package the application requires. A roughly 10-month review after that would put a decision in late 2027 at the earliest. The evidence base spans multiple trials across obesity, type 2 diabetes, and heart-disease populations: the flagship obesity trial (TRIUMPH-1) read out with strong results in May 2026, an earlier obesity plus knee-osteoarthritis trial reported in December 2025, two further obesity trials reported in July 2026, and a diabetes trial reported in March 2026. A separate legal dispute over whether retatrutide is regulated as a biologic could affect its market exclusivity, but is not expected to delay the approval decision itself. Approval will also depend on whether the dysesthesia signal can be managed at lower doses.
Recent newsletter coverage
Past pieces from the GLP-1 Observer newsletter that touched on this class.
- May 22, 2026 · Trial Spotlight: The 28% Drug, Now With a Dial: retatrutide's flagship Phase 3 TRIUMPH-1 confirms 28.3% weight loss at the top dose while revealing a dose ladder where the lowest dose still delivers nearly 20% with a discontinuation rate below placebo.
- May 22, 2026 · Mechanism Explained: Three Levers at Once: why pairing the appetite suppression of GLP-1 and GIP with glucagon's energy-out, liver-fat-burning lever lets a triple agonist push past the 16 to 22% ceiling where the best duals plateau.
References
- Drucker DJ. GLP-1-based therapies for diabetes, obesity and beyond. Nature Reviews Drug Discovery. 2025.
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial. New England Journal of Medicine. 2023. (Phase 2 pivotal obesity trial)
- Rosenstock J, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial conducted in the USA. The Lancet. 2023. (Phase 2 type 2 diabetes trial)
- Sanyal AJ, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nature Medicine. 2024. (Phase 2a liver-disease trial)
- Giblin K, et al. Retatrutide for the treatment of obesity, obstructive sleep apnea and knee osteoarthritis: Rationale and design of the TRIUMPH registrational clinical trials. Diabetes, Obesity and Metabolism. 2026. (Phase 3 program design)
Track this class
GLP-1 Observer tracks clinical trials, news, and regulatory milestones across the GLP-1 and obesity-drug landscape, updated daily. See trial timelines, date-change alerts, and weekly roll-ups.