GLP-1 + Amylin Combinations
Drugs that pair two appetite-suppressing hormones, either by mixing two molecules or by engineering one that binds both receptors.
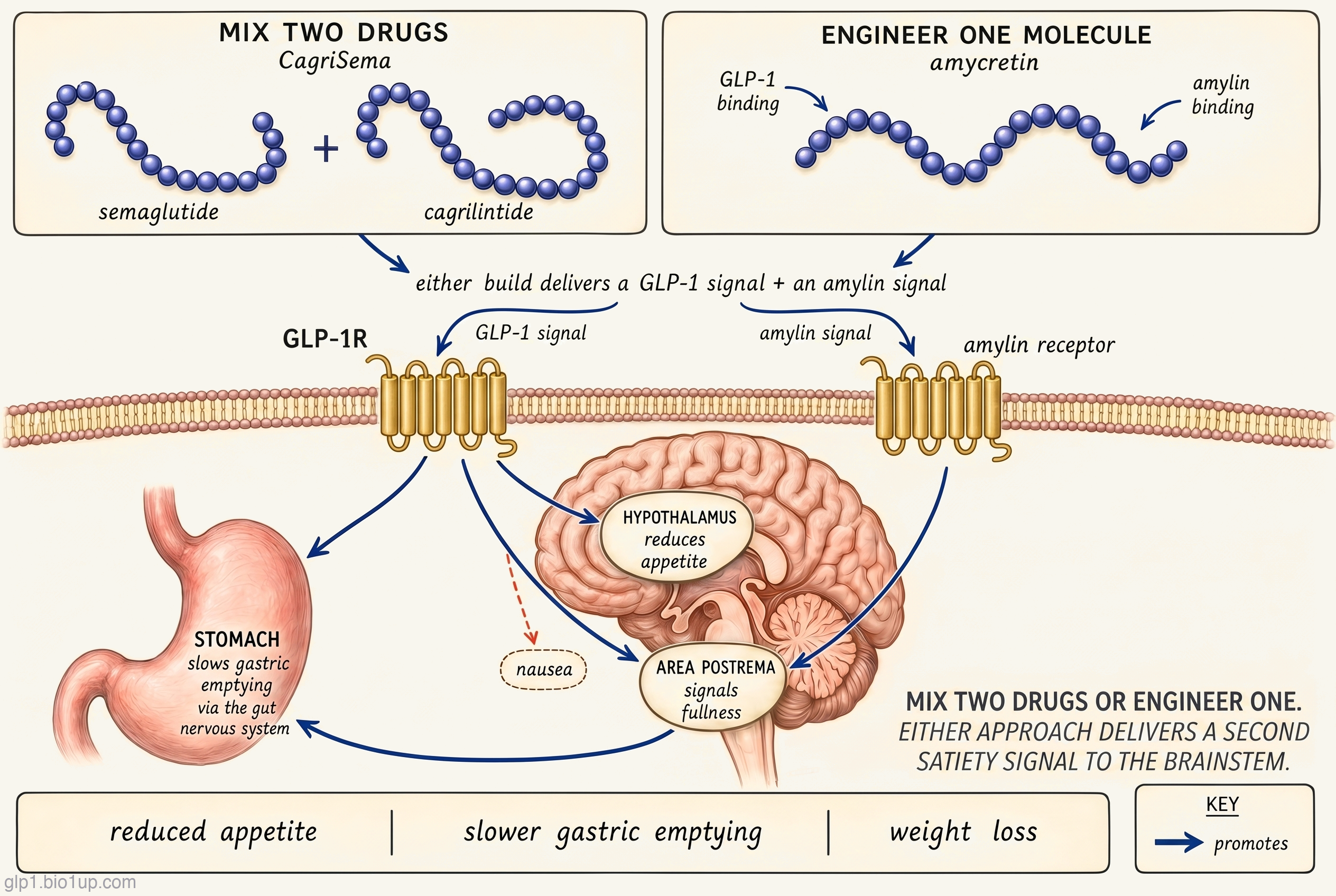
GLP-1 dulls hunger and the urge to eat. Amylin, a hormone the pancreas releases alongside insulin, signals fullness through different brain circuits. Combining the two gives both signals. Two ways to build that combination exist: mix two drugs, or engineer one that binds both receptors.
No GLP-1 + amylin combination is approved as of July 2026, but CagriSema (Novo Nordisk) is under FDA review after Novo filed its New Drug Application in December 2025. Amycretin, Novo's unimolecular co-agonist, is also in Phase 3. The class's central question is whether engineering one molecule that binds both receptors (amycretin) turns out meaningfully better than mixing two drugs in one injection (CagriSema).
Re-checked August 3, 2026
Every claim on this page is re-verified against sources including ClinicalTrials.gov, regulatory actions, press releases, and the published literature, all tracked in the GLP-1 Observer database.
GLP-1 + amylin combinations are a class of obesity drugs that activate two appetite-regulating hormone receptors at the same time. GLP-1, the target of Ozempic and Wegovy, reduces hunger and slows how quickly food leaves the stomach. Amylin, a less well-known hormone released from the pancreas alongside insulin, suppresses appetite through different brain pathways. Combining the two signals has become one of the most serious challenges to the pure-GLP-1 franchise. Novo Nordisk has two programs in Phase 3 (CagriSema and amycretin), AstraZeneca has a program in Phase 2, and Metsera (acquired by Pfizer in 2025) has a program in Phase 2. Together, these programs are testing whether combining GLP-1 with amylin can beat tirzepatide's efficacy, preserve more lean muscle than GLP-1 alone, or both. There are two structural approaches in the class: combining two separate molecules, or engineering a single molecule that activates both receptors. Most programs combine two separate molecules; amycretin is the exception. The comparison between these two bets (both pursued by Novo Nordisk, with the same target pair) is the cleanest natural experiment the class has produced.
How GLP-1 + amylin combinations work
GLP-1 and amylin are two of the gut-brain signals the body uses to bring a meal to a close. They are biologically different molecules, act on different receptors, and reach the brain through different pathways. But the downstream effect they share is regulation of appetite.
GLP-1 (glucagon-like peptide-1) is released from specialized cells in the small intestine after a meal. Its main jobs are to tell the pancreas to release insulin in proportion to the glucose that just arrived, to slow how quickly food leaves the stomach, and to signal fullness to the brain. Mono-agonist drugs like semaglutide (sold as Ozempic for diabetes and Wegovy for obesity) copy this signal at doses and durations well above anything the body produces on its own, which is where the weight loss comes from. The biggest appetite-reducing effect operates through receptors in the hypothalamus and reward-processing regions of the brain.
Amylin is released from pancreatic beta cells, co-secreted with insulin whenever those cells sense the rise in blood sugar that follows a meal. GLP-1 comes from a different tissue entirely: specialized L-cells in the small intestine, which detect nutrients directly as food arrives. So the two signals are parallel satiety cues from two different meal-sensing organs, reaching the brain on different timing. Amylin's main jobs are to slow gastric emptying further (on top of what GLP-1 already does, mediated centrally rather than at the gut directly), to suppress post-meal glucagon release, and, most importantly for the obesity question, to signal satiety through a different brain circuit than GLP-1. While GLP-1 acts broadly across multiple brain regions (including both the hypothalamus and the brainstem), amylin acts more specifically on the area postrema in the brainstem. The two pathways are thought to be additive, and the breadth difference is part of why combining them produces effects neither hormone reaches alone.
Amylin is not a simple receptor story. The amylin receptor itself is a complex, built by combining the calcitonin receptor with one of three small helper proteins called RAMPs (receptor activity-modifying proteins). The pairing changes what the receptor binds and how it signals. Cagrilintide, the amylin agonist in CagriSema, is technically a dual amylin and calcitonin receptor agonist because it engages both the calcitonin receptor alone and the amylin-receptor complex that includes it. Clinically, the story is simpler: in patients, cagrilintide's effects (appetite suppression, slower gastric emptying, weight loss) match what you'd expect from the amylin pathway alone, without distinct calcitonin-mediated effects on calcium or bone.
A GLP-1 + amylin combination delivers both the GLP-1 and amylin signals together. The two hypotheses for why this matters are that the added amylin signal (1) produces more weight loss than GLP-1 alone by adding a second satiety circuit, and (2) preserves more lean mass than GLP-1 alone, by slowing the metabolic shift that drives muscle loss during weight loss. The first hypothesis is being tested directly by the Phase 3 programs. The second is being tested by DEXA (body-composition) substudies, and the early human data has not yet borne it out.
Where the class is evolving
This class is young enough that the live questions still outnumber the settled answers. A few stand out in the current pipeline.
Two structural bets on the same target pair
The cleanest natural experiment in the class is Novo Nordisk's own two programs: CagriSema and amycretin, both activating GLP-1 and amylin, but built in structurally distinct ways.
CagriSema is a fixed-dose combination: semaglutide (the GLP-1 agonist in Ozempic and Wegovy) and cagrilintide (a long-acting amylin agonist) in one weekly injection. Each component was developed as a standalone drug. They are mixed at a fixed ratio in the finished product.
The advantage is a known GLP-1 backbone. Semaglutide has years of safety data and a familiar side-effect profile. The tradeoff is that the pharmacology is inherited rather than designed from scratch: Novo chooses the dose ratio between semaglutide and cagrilintide, but the individual molecules' potencies and pharmacokinetics are fixed by their existing structures.
Amycretin is a single peptide designed to activate both the GLP-1 receptor and the amylin receptor. It is one molecule with two binding surfaces, not two drugs mixed together.
The advantage is that the molecule's properties can be designed from scratch: Novo can choose its potency at each receptor and its pharmacokinetics, while CagriSema's properties are inherited from the existing semaglutide and cagrilintide molecules. Amycretin is also being developed in both injectable and oral formulations, whereas CagriSema is injection-only.
Both programs are from the same company, both are in Phase 3, and both produce broadly similar weight loss in early data. The question Novo (and obesity researchers more broadly) is trying to answer is whether the engineered-single-molecule approach turns out to be cleaner in the long run (tolerability, flexibility across doses, route of administration), or whether the fixed-dose combination is close enough that the engineering work isn't worth the delay it adds.
The muscle-sparing hypothesis
The clinical pitch for adding amylin to GLP-1 is not primarily that it produces more weight loss. It is that the weight lost with the combination is better weight, with more of the loss coming from fat and less from lean mass. Every obesity drug tested to date loses some lean mass along with fat, which is unsurprising (any meaningful weight loss does, by diet or drug). Whether amylin's addition meaningfully changes that ratio is the question body-composition substudies (using DEXA) are built to answer, and the first of those readouts has now arrived.
This matters clinically because muscle mass tracks with physical function, metabolic rate, and long-term outcomes. A drug that produces the same total weight loss as semaglutide but with a better fat-to-lean-mass ratio would be a meaningful improvement even without a higher headline number. The biological argument is plausible (amylin influences metabolic rate and has been studied for years as a body-composition signal in animal models), but the first human data has not yet borne it out. The peer-reviewed REDEFINE-1 paper published in 2025 reported body composition only against placebo, not a head-to-head comparison against the trial's semaglutide arm, and when a DEXA sub-analysis was presented at the European Congress on Obesity in May 2026, it showed that CagriSema's weight loss came mostly from fat with muscle strength preserved, but did not show the combination sparing more lean mass than semaglutide alone. If anything, semaglutide's loss in that trial was marginally more fat-predominant. As of July 2026, the claim that adding amylin spares more muscle than GLP-1 by itself remains a mechanistic hypothesis that early data has not yet supported, and the comparison against the semaglutide arm still awaits peer-reviewed publication.
Dosing-interval engineering
The current standard for injectable obesity drugs is once-weekly. Amylin agonists developed to date (cagrilintide, AZD6234, MET-233) have been designed to match that cadence. Metsera's MET-097 + MET-233 combination is the program exploring a step further: both components are designed to be ultra-long-acting, with the goal of extending the dosing interval to monthly. Whether a monthly injection is meaningfully different from a weekly one for adherence is still an open clinical question. Some patients prefer less-frequent dosing, others prefer the weekly rhythm. Amgen's MariTide is testing the same monthly-or-less-frequent concept further along (in another class entirely, and as a different mechanism); within the GLP-1 + amylin class, the Metsera program is the first serious test.
The competitive landscape
Landscape as of July 2026No GLP-1 + amylin combination is approved yet, but CagriSema is under FDA review as of July 2026. Its first Phase 3 readout (REDEFINE-1, in obesity) reported in December 2024 with 22.7% average weight loss on the top dose over 68 weeks. The result was clinically meaningful on its own, but it essentially matched tirzepatide's 22.5% rather than clearly beating it, and it fell short of the "at least 25%" bar Novo's management had guided investors toward. Novo's shares dropped sharply on the day of the announcement. A second readout, REDEFINE-2, reported in 2025 in patients with both obesity and type 2 diabetes, with a somewhat smaller 15.7% weight loss, reflecting the pattern seen across the obesity-drug class in patients with both conditions. Novo filed the New Drug Application with the FDA in December 2025 and now guides a US regulatory decision in the fourth quarter of 2026, which would clear the way for a launch in early 2027 if the review is positive.
Amycretin (which Novo Nordisk now formally calls zenagamtide) is Novo's second swing. Two early-phase papers published in The Lancet in 2025 established the profile: the injectable formulation produced up to 24% weight loss over 36 weeks at the top dose, and the oral formulation produced around 13% over 12 weeks. Novo advanced amycretin to Phase 3 on the strength of those results. Both the injectable and oral formulations have now reached Phase 3, but the injectable formulation is further along. Whether the engineered-single-molecule approach produces meaningfully different efficacy or tolerability than the CagriSema fixed-dose combination is the class's central open question.
AstraZeneca is the clearest challenger outside Novo. Its AZD9550 + AZD6234 program pairs AZ's own GLP-1 / glucagon dual agonist with a selective amylin agonist, effectively covering three hormone pathways. The Phase 2b trial reached primary completion in May 2026, with a topline readout expected in the second half of the year. Because AZD9550 activates the glucagon receptor alongside GLP-1, the combination's pharmacology is closer to a three-hormone cocktail than a pure GLP-1 + amylin pair, and it should be read that way.
Metsera's MET-097 + MET-233 is the furthest back, in Phase 2 as of July 2026, and its deal history is a more interesting story than its data yet. After a fall 2025 bidding war with Novo Nordisk, Pfizer acquired Metsera in November in a deal worth up to roughly $10 billion (nearly double its September offer), winning partly on antitrust-clearance grounds. The program's differentiating bet is not peak efficacy but dosing interval: both components are engineered to be ultra-long-acting, so the combination could eventually be injected once a month instead of weekly.
The race to watch over the next 12 to 18 months: whether CagriSema earns FDA approval and what the label will say, whether amycretin's Phase 3 results come in meaningfully better than CagriSema's, whether DEXA body-composition substudies across the class show a real muscle-sparing advantage, and whether AZ's three-pathway combination justifies its structural complexity once Phase 2 results arrive.
Drugs in this class
| Drug | Developer | Formulation | Stage | Conditions |
|---|---|---|---|---|
| CagriSema | Novo Nordisk | Weekly injection (fixed-dose semaglutide + cagrilintide) | Phase 3 (NDA filed) | Obesity, type 2 diabetes |
| Amycretin | Novo Nordisk | Weekly injection and daily oral (unimolecular co-agonist) | Phase 3 | Obesity |
| AZD9550 + AZD6234* | AstraZeneca | Weekly injection (dual agonist + amylin agonist, separately dosed) | Phase 2 | Obesity |
| MET-097 + MET-233 | Metsera (Pfizer) | Monthly injection (ultra-long-acting GLP-1 + amylin, separately dosed) | Phase 2 | Obesity |
* AZD9550 is itself a GLP-1 / glucagon dual agonist, so the combination covers three hormone pathways (GLP-1, glucagon, and amylin) rather than two. Included here because the program is tracked in the GLP-1 + amylin combination bucket based on the addition of the amylin component to a GLP-1 backbone.
Related and adjacent mechanisms
A few related drug classes don't quite fit the GLP-1 + amylin combination definition but sit close enough to be worth knowing about, especially if you're trying to understand where obesity medicine might be heading.
Pair GLP-1 with a different second receptor: GLP-1 / GIP and GLP-1 / glucagon duals
Adding a second receptor target to a GLP-1 backbone is the core move of the entire "beyond GLP-1" field, and amylin is one of the partners being tested alongside GIP and glucagon. The GLP-1 / GIP duals (tirzepatide and its challengers) are the most established, with tirzepatide already on the market. The GLP-1 / glucagon duals (survodutide, pemvidutide, mazdutide) are further behind but showing strong liver-disease effects alongside weight loss. Each pairing bets on different downstream physiology: GIP on insulin amplification, glucagon on energy expenditure, amylin on additional satiety and muscle sparing. Head-to-head data across these pairings doesn't exist yet, so which second receptor turns out to be the best partner for GLP-1 is still an open field question.
Add a third receptor: triple agonists
A triple agonist activates GLP-1, GIP, and glucagon with a single molecule. Eli Lilly's retatrutide is the lead drug in that class. Its flagship Phase 3 obesity trial, TRIUMPH-1, read out in May 2026 with 28.3% average weight loss at the top dose, the largest any obesity drug has shown in a pivotal trial to date. Triples represent a different direction from amylin combinations: adding complexity inside the incretin axis rather than stepping outside it to recruit amylin's separate brain pathway. Both bets are live.
Isolate the satiety signal: amylin mono agonists
Amylin-only programs are a full competitive landscape in their own right. Cagrilintide (Novo Nordisk, in the RENEW program) and eloralintide (Eli Lilly, in the ENLIGHTEN program) are both in Phase 3 as stand-alone amylin agonists for obesity. Zealand Pharma's petrelintide (partnered with Roche) and AstraZeneca's AZD6234 are in Phase 2, with earlier-stage programs from Pfizer, AbbVie / Gubra, and others behind them. The class is usually positioned as either an add-on to GLP-1 therapy or, if monotherapy Phase 3 data delivers, as a differentiated option for patients who don't tolerate GLP-1 drugs. Pramlintide (Symlin), an older amylin analog approved as a diabetes adjunct, remains in use for specific indications.
For how CagriSema stacks up beyond the mechanism, the GLP-1 Verdict grades it on efficacy and tolerability: see its Verdict page.
Frequently asked questions
What is a GLP-1 + amylin combination?
A GLP-1 + amylin combination is an obesity drug that activates two appetite-regulating hormone receptors at once: the GLP-1 receptor (the same target as Ozempic and Wegovy) and the amylin receptor. GLP-1 and amylin are both signals the body uses after a meal to reduce appetite and slow digestion, but they act through different brain pathways, so combining them is expected to add satiety effects rather than duplicate them. Two structural approaches exist: combining two separate molecules (CagriSema is the lead example), or a single engineered molecule that binds both receptors (amycretin is the lead example). No drug in this class is approved yet.
How is amycretin different from CagriSema?
Both drugs activate the same two receptors (GLP-1 and amylin) and are developed by the same company (Novo Nordisk). The difference is structural. CagriSema is two separate drugs (semaglutide and cagrilintide) combined at a fixed ratio in one injection. Amycretin is a single peptide engineered to bind both receptors itself. The engineered molecule can be tuned for specific receptor potencies and is being developed in both injectable and oral formulations, while CagriSema is injection-only. Early clinical efficacy has been broadly similar. Whether amycretin's structural advantages translate into meaningfully better tolerability or efficacy in Phase 3 is the class's central open question.
Does adding amylin preserve muscle during weight loss?
The honest answer is that we do not yet know it spares more muscle than GLP-1 alone. Every obesity drug produces some lean-mass loss alongside fat loss, because meaningful weight loss of any kind does. The clinical hypothesis for adding amylin to GLP-1 is that the combination produces a better fat-to-lean-mass ratio than GLP-1 alone, based on amylin's distinct effects on metabolic rate and body composition. The first test came from a DEXA sub-analysis of CagriSema's REDEFINE-1 trial, presented in May 2026: most of the weight lost was fat and muscle strength was preserved, but the combination did not spare more lean mass than semaglutide on its own. As of July 2026, the muscle-sparing case for the class rests on biological plausibility rather than head-to-head evidence: the published REDEFINE-1 paper reported body composition only against placebo, and the comparison against the semaglutide arm still awaits peer-reviewed publication. Larger and longer Phase 3 readouts may yet settle it.
Why was CagriSema's first Phase 3 readout a disappointment?
CagriSema's REDEFINE-1 result in December 2024 produced 22.7% average weight loss on the top dose over 68 weeks, which in absolute terms is one of the strongest weight-loss results any obesity drug has produced. The disappointment was relative, not absolute. Novo had guided investors toward "at least 25%" pre-readout, and competitive expectations had been set by tirzepatide's 22.5% pivotal obesity result and retatrutide's Phase 2 results of roughly 24%. CagriSema's result essentially matched tirzepatide rather than clearly beating it and came in below the pre-readout bar, and Novo's stock dropped sharply on the day of the announcement. The market read the miss as a sign that the fixed-dose combination didn't deliver the full synergy the mechanism implied. These are efficacy estimates (average weight loss in trial participants who stayed on the drug through the end of the study; real-world numbers, which include patients who stop, run a few percentage points lower).
When will a GLP-1 + amylin combination be approved?
CagriSema has the first realistic chance. Novo filed the New Drug Application with the FDA in December 2025 and now guides a US regulatory decision in the fourth quarter of 2026, which would clear the way for a launch in early 2027 if the review runs smoothly. Amycretin is behind CagriSema in Phase 3 but not dramatically; a 2027 or 2028 filing is plausible if the registrational trials run cleanly. AstraZeneca's AZD9550 + AZD6234 program and Pfizer / Metsera's MET-097 + MET-233 are several years behind and are not realistic near-term candidates.
Recent newsletter coverage
Past pieces from the GLP-1 Observer newsletter that touched on this class.
- May 29, 2026 · Trial Spotlight: A Plan B for GLP-1 Intolerance - Novo Tests Cagrilintide on Its Own: a standalone Phase 1 of cagrilintide aimed at people who came off GLP-1s for GI side effects, with a tolerability primary endpoint that signals a separate amylin franchise beyond CagriSema.
- May 8, 2026 · Trial Spotlight: Three Ways to Build a GLP-1 + Amylin Combo: Novo and Pfizer register combo trials contrasting three molecular architectures: amycretin's unimolecular co-agonist and CagriSema's fixed-ratio single device (both Novo, Phase 3) versus Pfizer's Phase 2 pairing of separately dosed MET-097 plus MET-233.
- April 24, 2026 · Mechanism Explained: Amycretin and the Amylin Selectivity Problem: why amylin receptor selectivity (AMYR versus the calcitonin receptor) splits the field into broad agonists like cagrilintide and petrelintide versus selective agonists like eloralintide, and where amycretin's unimolecular design fits.
References
- Garvey WT, et al. Coadministered cagrilintide and semaglutide in adults with overweight or obesity. New England Journal of Medicine. 2025. (REDEFINE-1 Phase 3 obesity trial)
- Davies MJ, et al. Cagrilintide-semaglutide in adults with overweight or obesity and type 2 diabetes. New England Journal of Medicine. 2025. (REDEFINE-2 Phase 3 trial)
- Enebo LB, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2.4 mg for weight management: a randomised, controlled, phase 1b trial. The Lancet. 2021. (CagriSema Phase 1b combination dose-finding)
- Gasiorek A, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of the first-in-class GLP-1 and amylin receptor agonist, amycretin: a first-in-human, phase 1, double-blind, randomised, placebo-controlled trial. The Lancet. 2025. (Amycretin oral Phase 1)
- Dahl K, et al. Amycretin, a novel, unimolecular GLP-1 and amylin receptor agonist administered subcutaneously: results from a phase 1b/2a randomised controlled study. The Lancet. 2025. (Amycretin subcutaneous Phase 1b/2a)
Track this class
GLP-1 Observer tracks clinical trials, news, and regulatory milestones across the GLP-1 and obesity-drug landscape, updated daily. See trial timelines, date-change alerts, and weekly roll-ups.