GLP-1 / Glucagon Dual Agonists
A fat-burning lever paired with GLP-1's appetite suppression, still in trials, with unusual reach into liver disease.
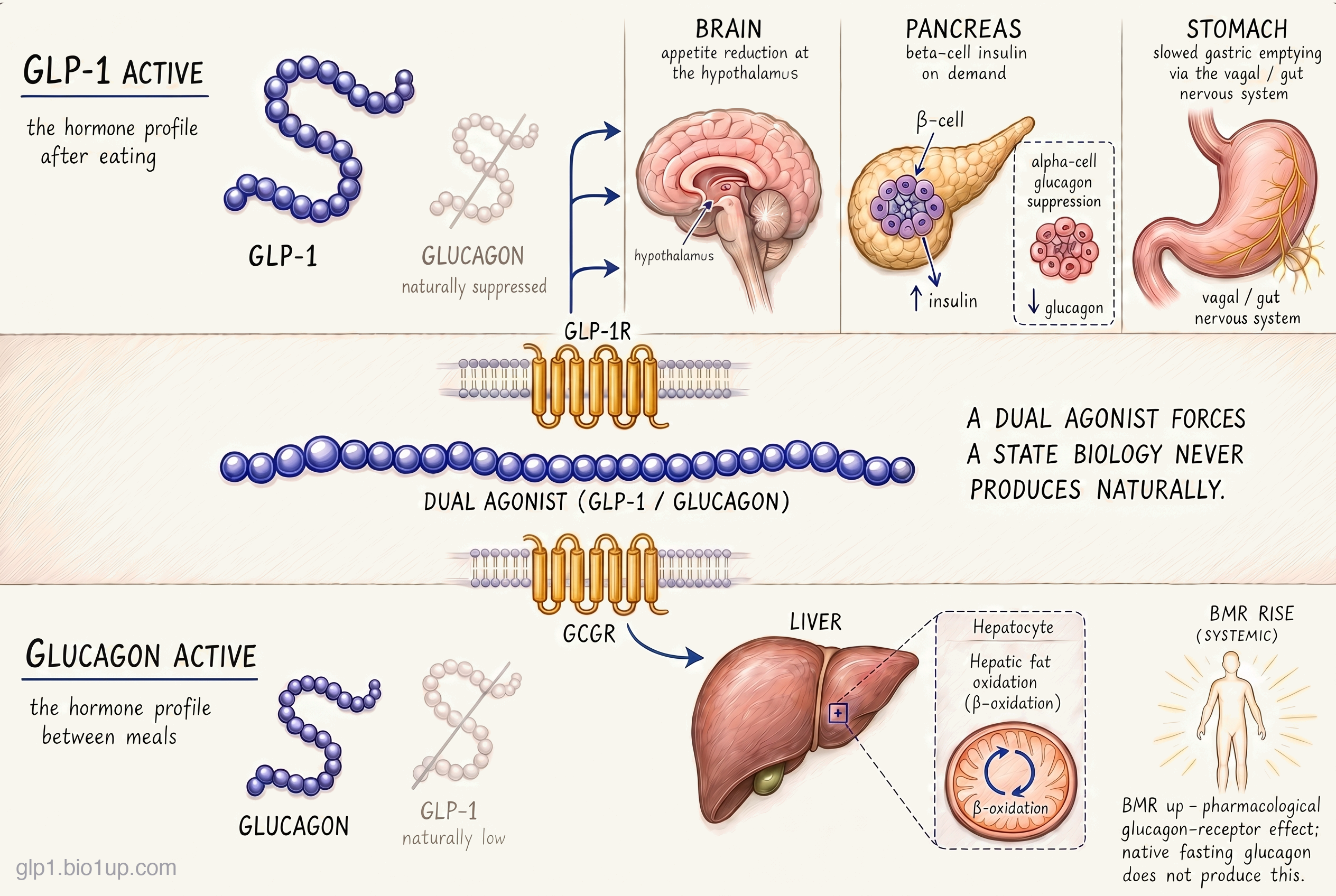
GLP-1 suppresses appetite. Glucagon tells the body to burn more of what's already stored. A GLP-1 / glucagon dual agonist combines these effects in a single molecule.
Counts reflect publicly disclosed programs in our database. Earlier-stage or undisclosed assets may not yet be represented. No drugs in this class are approved in the US or EU as of July 2026; mazdutide (Innovent, brand name Xinermei) is approved only in China.
Re-checked August 3, 2026
Every claim on this page is re-verified against sources including ClinicalTrials.gov, regulatory actions, press releases, and the published literature, all tracked in the GLP-1 Observer database.
GLP-1 / glucagon duals are an obesity drug class that explicitly targets liver disease alongside weight loss. One approved drug sits in the class today: mazdutide, approved in China in 2025. No drugs are yet approved in the US or EU. Behind mazdutide, survodutide from Boehringer Ingelheim is in global Phase 3 for both obesity and liver disease, and Merck's efinopegdutide and Altimmune's pemvidutide are in Phase 2. AstraZeneca's cotadutide, once the flagship candidate in the class, was discontinued in 2023. The unifying mechanism is simple and counterintuitive: add a carefully tuned glucagon signal on top of GLP-1 to force a state the body never naturally enters, pairing the appetite suppression of the fed state with the fat-burning glucagon signal normally reserved for fasting.
How GLP-1 / glucagon duals work
The first thing to square is the paradox. Glucagon is the hormone you associate with raising blood sugar: the injection paramedics give someone in a hypoglycemic crisis. Why would an obesity drug add that?
The answer is dose and duration. A short, strong pulse of glucagon raises blood sugar by pulling glucose out of the liver, which is exactly what rescues someone mid-hypoglycemia. A low, sustained glucagon signal does something different. It raises resting energy expenditure (the calories your body burns just keeping itself running) and mobilizes fat out of the liver. Paired with GLP-1 (glucagon-like peptide-1), which keeps insulin working normally and suppresses appetite, the glucagon signal becomes a fat-burning lever rather than a glycemic problem. GLP-1 handles the input side (you eat less); glucagon handles the output side (you burn more of what's already stored).
A GLP-1 / glucagon dual agonist is a single peptide molecule designed to activate both receptors at once. GLP-1 at its receptors in the pancreas, stomach, and brain produces the familiar effects of the mono class: glucose-dependent insulin release, delayed gastric emptying, and reduced appetite. Glucagon at its receptor, which sits predominantly on liver cells (hepatocytes), drives hepatic fat oxidation (the liver burns its own stored fat for energy) and raises whole-body basal metabolic rate by a few percent. In obesity trials, the compound effect is weight loss at least comparable to the strongest GLP-1 mono agonists. In liver disease trials, the effect on hepatic fat content is larger than GLP-1 alone can achieve, which is part of why the FDA has granted Breakthrough Therapy designation (BTD) to two drugs in this class (survodutide and pemvidutide) for MASH (metabolic dysfunction-associated steatohepatitis, the liver disease formerly called NASH).
The catch is a real one. The ratio of GLP-1 to glucagon activity has to be tuned carefully: too much glucagon relative to GLP-1 and blood sugar rises in patients whose beta cells can't compensate; too little and you lose the liver and metabolic-rate advantage. Different drugs in this class have taken different positions on that spectrum, and some early candidates failed specifically on this tuning. How that plays out is below.
Where the class is evolving
The GLP-1 / glucagon dual class is mid-flight. One drug is approved in China, the global Phase 3 programs are still running, and the first US and EU approvals are years away. Three developments shape where the class is going.
The ratio between GLP-1 and glucagon is the class's signature dial
Every drug in this class has to decide how much glucagon activity to build in relative to GLP-1 activity. The choice is a real pharmacological dial, usually expressed as a GLP-1-to-glucagon potency ratio. Drugs sit along a spectrum from heavily GLP-1-leaning at one end to more glucagon-leaning at the other, and where a molecule lands shapes what it is good at.
Pemvidutide is explicitly engineered at a 1-to-1 GLP-1-to-glucagon potency ratio. The pitch: give equal weight to appetite suppression and to the energy-expenditure and liver-fat effects that glucagon contributes.
IMPACT Phase 2b in MASH met its 24-week primary endpoint in June 2025 (MASH resolution without fibrosis worsening in 52 to 58% of patients versus 20% on placebo). FDA BTD in MASH followed in January 2026.
Survodutide is heavily weighted toward the GLP-1 side, with an in vitro potency ratio of roughly 8:1 GLP-1-to-glucagon. The rationale: lean on GLP-1 for appetite suppression and glycemic control, then add a controlled amount of glucagon activity to capture the energy-expenditure and hepatic-fat benefits without risking hyperglycemia in patients whose beta cells are stressed.
FDA BTD in MASH was granted in October 2024. The global Phase 3 program runs in parallel for obesity and for liver disease. Phase 2 data showed up to 18.7% weight loss at 46 weeks.
The trade-off is not settled. Drugs further toward the glucagon end in principle deliver larger liver-fat and energy-expenditure effects, but risk worse glycemic tolerability in patients whose beta cells are already stressed. Drugs further toward the GLP-1 end behave closer to a GLP-1 mono, with a smaller (but, the field hopes, still meaningful) liver and metabolic-rate bonus. Both pemvidutide and survodutide have reached MASH BTD even from very different ratios, which suggests the right ratio is still an open question. The Phase 3 readouts over the next 12 to 24 months will start to settle which positions on the dial deliver the best combination of weight loss, liver benefit, and tolerability.
A first approval in China, ahead of the US and EU
Mazdutide (Innovent Biologics, brand name Xinermei) became the first GLP-1 / glucagon dual agonist approved anywhere when China's National Medical Products Administration (NMPA) cleared it for chronic weight management in June 2025. A type 2 diabetes indication followed in September 2025. A higher-dose version is under NMPA review, supported by trial data showing weight loss up to about 20% of baseline.
This is a notable wrinkle for a field where US and EU regulators have historically approved GLP-based drugs first. Mazdutide has been developed primarily in a Chinese trial program, and for US and EU patients the wait continues, with no filings yet.
Earlier candidates got caught on the ratio
The class has real attrition. Cotadutide, an AstraZeneca drug, was the first-generation flagship and the drug most responsible for validating the GLP-1 / glucagon dual concept in early clinical trials. AstraZeneca discontinued it in 2023 in favor of a once-weekly successor (the cotadutide formulation required daily dosing, which had become inconvenient in a field that moved to weekly injections). An earlier candidate from Johnson & Johnson hit its weight-loss endpoint in Phase 2 but, in the parallel type 2 diabetes study, failed to improve glycemic control; J&J returned the asset in 2019. Hanmi reclaimed rights and re-licensed to Merck, where it continues in development as efinopegdutide, focused primarily on liver disease.
These stumbles shaped the class. Every drug still in development is weekly or less frequent in dosing, and each has made a deliberate decision about where on the GLP-1-to-glucagon ratio spectrum to land. The Withdrawn and paused section at the bottom of this page describes what is no longer in development.
Liver disease is the second indication that defines this class
MASH (metabolic dysfunction-associated steatohepatitis, formerly called NASH) is a liver disease in which fat buildup drives inflammation, scarring, and eventually cirrhosis or liver failure. It is closely linked to obesity and type 2 diabetes, and until recently had almost no approved therapy.
GLP-1 / glucagon duals work on it better than GLP-1 mono agonists do. The mechanism explains why: glucagon at its receptor directly reduces the fat stored in liver cells, while GLP-1 drugs help MASH primarily indirectly through weight loss. In clinical trials, the effect on liver fat from a dual agonist has been larger than GLP-1 alone can achieve.
Five programs in this class are in active MASH development: survodutide (in Phase 3 with FDA BTD), pemvidutide (Phase 2 with FDA BTD, Phase 3 planned for 2026), efinopegdutide from Merck (Phase 2), DD01 from D&D Pharmatech (Phase 2), and mazdutide from Innovent Biologics (Phase 2). With survodutide's SYNCHRONIZE-1 Phase 3 obesity trial having read out in April 2026 while its registrational MASH outcome data remains years away, an obesity approval for the class may now arrive before liver disease, reversing the earlier expectation.
The competitive landscape
Landscape as of July 2026No obesity drug in this class is approved in the US or EU as of July 2026. The pipeline is unusually international, and companies fall into three broad groups.
Innovent Biologics is the first mover, with mazdutide approved in China for obesity and type 2 diabetes. Boehringer Ingelheim and Zealand Pharma run the largest global program, with survodutide in Phase 3 for both obesity and MASH. Altimmune and Merck sit behind them with pemvidutide and efinopegdutide, both in Phase 2 and both focused first on liver disease. Other Chinese programs could eventually follow Innovent's path through the NMPA; AstraZeneca is rebuilding in the class with a once-weekly successor to the discontinued cotadutide.
Survodutide's Phase 3 obesity readout is now in: up to 16.6% weight loss at 76 weeks if taken as prescribed, and up to 13% on the treatment-regimen estimand that counts everyone who started (the treatment-regimen figure was first disclosed at ADA 2026). On the efficacy estimand, the 16.6% trails tirzepatide at 22.5% and the triple agonist retatrutide at 28.3% (its Phase 3 TRIUMPH-1 readout). A number this far back points the class toward a primarily liver-disease niche rather than a front-line obesity contender.
Drugs in this class
The table below covers active programs in the GLP-1 / glucagon dual class as of July 2026. The Withdrawn and paused section at the bottom covers the drugs that shaped the class's history but are no longer in development.
| Drug | Developer | Formulation | Stage | Conditions |
|---|---|---|---|---|
| Mazdutide (Xinermei) | Innovent Biologics | Weekly injection | Approved in China | Obesity, type 2 diabetes |
| Survodutide | Boehringer Ingelheim + Zealand Pharma | Weekly injection | Phase 3 | Obesity, liver disease |
| Pemvidutide | Altimmune | Weekly injection | Phase 2b | Liver disease, obesity |
| Efinopegdutide (MK-6024) | Merck | Weekly injection | Phase 2b | Liver disease |
| DD01 (zabopegdutide) | D&D Pharmatech | Weekly injection | Phase 2 | Liver disease |
Other programs
Other drugs in the class are also in development, with less public clinical data:
- AZD9550 (AstraZeneca): a once-weekly successor to the discontinued cotadutide, evaluated in the (now completed) Phase 2b ASCEND study both as monotherapy and in combination with the amylin analog AZD6234, with further Phase 2 studies ongoing.
- DA-1726 (MetaVia): a GLP-1 / glucagon dual in Phase 1 for obesity and liver disease.
Withdrawn and paused
One drug that shaped the class's early history is no longer in development.
- Cotadutide (AstraZeneca) was the first-generation flagship and the drug most responsible for establishing that a GLP-1 / glucagon dual could produce real weight loss and liver-fat effects in humans. AstraZeneca discontinued it in 2023 because its daily dosing profile had become inconvenient relative to weekly competitors, and pivoted resources to the once-weekly AZD9550.
Cotadutide's exit shaped the current generation. Every drug still in development is weekly or less frequent in dosing, and each has made a deliberate decision about where on the GLP-1-to-glucagon ratio to land.
Related and adjacent mechanisms
Several nearby classes share mechanism with GLP-1 / glucagon duals or sit next to them in the obesity and liver-disease pipeline. None of them is a GLP-1 / glucagon dual, but each is close enough that readers comparing options will encounter them.
Add a third receptor: triple agonists
Adding a third receptor (GIP) to a GLP-1 / glucagon dual produces a triple agonist, which is the mechanism of retatrutide (Eli Lilly, Phase 3 for obesity). A triple agonist carries the same logic as a GLP-1 / glucagon dual (GLP-1 for appetite, glucagon for energy expenditure and liver fat) and adds GIP-receptor activation, which in animals contributes additional insulin-sensitization and adipose-tissue effects. In the Phase 3 TRIUMPH-1 obesity trial (reported May 2026), retatrutide produced up to 28.3% weight loss at 80 weeks (12 mg, if taken as prescribed). That exceeds its ~24% Phase 2 result and is the highest reported for any GLP-1-based obesity drug to date. Triple agonists have their own field guide.
Pair GLP-1 with GIP instead: GLP-1 / GIP duals
Tirzepatide (Mounjaro for type 2 diabetes, Zepbound for obesity) is the best-studied dual agonist in obesity, but its second receptor is GIP, not glucagon. GLP-1 / GIP duals compete with the GLP-1 / glucagon duals for the same "bigger than mono-agonist weight loss" positioning, but they do it through a different second mechanism (GIP instead of glucagon). GIP contributes to appetite regulation and to tolerability (GIP activation appears to reduce some of the nausea that GLP-1 causes); it does not have the direct liver-fat and energy-expenditure effects that glucagon does. The two classes are not substitutes for each other in MASH, and the competition between them in obesity is still being worked out.
Compare to the foundation: GLP-1 mono agonists
GLP-1 mono agonists are the foundational class against which every GLP-1 / glucagon dual is measured. Semaglutide at top doses can produce weight loss up to about 21% in pivotal obesity trials (STEP UP, 7.2 mg: 20.7% trial-product estimand); GLP-1 / glucagon duals need to at least match that efficacy while adding their distinct liver and metabolic-rate benefits. The GLP-1 mono field guide covers this class in detail.
Engage a different satiety hormone: amylin and GLP-1 + amylin combinations
Amylin analogs (such as cagrilintide, a component of CagriSema) and combination drugs that pair GLP-1 with amylin or other satiety-related peptides are a separate pharmacological approach to obesity. They work on different receptors and share no mechanism with glucagon. They are covered in the amylin combinations field guide.
For how survodutide stacks up beyond the mechanism, the GLP-1 Verdict grades it on efficacy and tolerability: see its Verdict page.
Frequently asked questions
Isn't glucagon the hormone that raises blood sugar? Why would an obesity drug add it?
The short answer is dose and duration. A rescue dose of glucagon (the injection given for severe hypoglycemia) is a pharmacological pulse that transiently mobilizes hepatic glucose to raise blood sugar, which is exactly what the patient needs in that moment. The glucagon activity in a GLP-1 / glucagon dual agonist is a sustained, low-level signal across the week between doses, very different from the rescue pulse. With sustained activation at this lower level, glucagon increases resting energy expenditure and drives hepatic fat oxidation. Paired with GLP-1 (which keeps insulin release intact and appetite low), the glucagon signal becomes a metabolic accelerator rather than a glycemic problem, provided the ratio is tuned correctly. Drugs that got that tuning wrong are exactly the ones that have been discontinued.
How does the weight loss from these drugs compare to tirzepatide or the future triple agonists?
Data to date suggest GLP-1 / glucagon duals at their best deliver weight loss in roughly the 15 to 20% range of baseline body weight (trial-product estimand; real-world and treatment-policy numbers run a few points lower). That puts the class roughly in line with the GLP-1 monos at their top doses and modestly behind tirzepatide (which reports about 22% at its top dose in obesity) and the triple agonist retatrutide (about 28% in its Phase 3 TRIUMPH-1 readout). The weight-loss edge of GLP-1 / glucagon duals over the mono class is real but smaller than the edge of the triple agonists, and the distinctive feature of the class is liver-disease activity, not record-breaking weight loss.
When will any of these be approved in the US?
Mazdutide is approved in China but not filed in the US or EU. Survodutide is the most advanced drug in the class globally; its Phase 3 obesity readout has now reported (SYNCHRONIZE-1, up to 16.6% at 76 weeks on the efficacy estimand), while its registrational MASH outcome trials do not complete until 2029 and 2031. The first US approval may therefore come in obesity rather than liver disease; a realistic earliest is around late-2028.
What is MASH and why is this class particularly good at it?
MASH (metabolic dysfunction-associated steatohepatitis, formerly called NASH) is a liver disease in which fat accumulates in the liver and drives inflammation, scarring, and eventually cirrhosis or liver failure. It is closely linked to obesity and type 2 diabetes. Glucagon receptor activation directly reduces fat stored in liver cells, which GLP-1 mono agonists do primarily indirectly through weight loss. This is part of why two drugs in this class (survodutide and pemvidutide) have received FDA Breakthrough Therapy designation specifically for MASH; semaglutide (Wegovy 2.4 mg), a GLP-1 mono, also received an earlier Breakthrough Therapy designation for MASH and was granted FDA accelerated approval in August 2025, but the dual-mechanism class is positioned to deliver a larger direct-on-liver effect.
Are GI side effects better or worse than with a GLP-1 mono?
Nausea, vomiting, and diarrhea are still the dominant side effects, and for some drugs in this class the ceiling dose has been set by GI tolerability rather than by weight-loss efficacy. Direct comparisons are still limited. Survodutide's detailed Phase 3 obesity data, presented at ADA 2026, drew scrutiny for gastrointestinal discontinuations that ran higher than the GLP-1 monos; across the rest of the class, tolerability still looks broadly in line with GLP-1 mono agonists at equivalent weight-loss doses. Titration schedules and dose step-ups are as important here as for the monos.
Recent newsletter coverage
Past focused pieces from the GLP-1 Observer newsletter that touched on this class:
- May 29, 2026 · Mechanism Explained: The Liver Is Glucagon's Home Turf: why the class's clearest wins are landing in liver disease, drawing on the EASL 2026 fibrosis data from pemvidutide and DD01.
- May 1, 2026 · Trial Spotlight: Survodutide Reads Out at 16.6%: survodutide's Phase 3 obesity readout and how it compares with the GLP-1 monos and tirzepatide.
- October 10, 2025 · Mechanism Explained: Dual GLP-1/Glucagon Agonists: introduction to the dual-pathway logic (GLP-1 for appetite, glucagon for energy expenditure) that defines this class.
References
The references below anchor the specific claims in this page. They are deliberately selective; thousands of papers exist on the class, and this list covers the ones most useful to a reader who wants to go deeper on mechanism and current state.
- Romero-Gómez M, et al. A phase IIa active-comparator-controlled study to evaluate the efficacy and safety of efinopegdutide in patients with non-alcoholic fatty liver disease. Journal of Hepatology. 2023;79(4):888-897. (Head-to-head liver-fat data versus semaglutide: 72.7% vs 42.3% least-squares mean relative liver-fat reduction, efinopegdutide vs semaglutide, at 24 weeks. Motivates the mechanistic claim that adding glucagon to GLP-1 directly reduces hepatic fat.)
- Le Roux CW, et al. Glucagon and GLP-1 receptor dual agonist survodutide for obesity: a randomised, double-blind, placebo-controlled, dose-finding phase 2 trial. Lancet Diabetes & Endocrinology. 2024;12(3):162-173. (Phase 2 obesity precedent showing up to 18.7% weight loss.)
- Boehringer Ingelheim + Zealand Pharma press release. Boehringer receives US FDA Breakthrough Therapy designation and initiates two Phase III trials in MASH for survodutide. October 8, 2024. (Source for the BTD date, indication language, and Phase 3 initiation.)
- Altimmune press release. Altimmune Announces Positive Topline Results from the IMPACT Phase 2b Trial of Pemvidutide in the Treatment of MASH. June 26, 2025. (Source for the 52-59% MASH resolution figures.)
- Innovent Biologics press release. Innovent Announces Mazdutide First Dual GCG/GLP-1 Receptor Agonist Received Approval from China's NMPA for Chronic Weight Management. June 2025. (Source for the first approved GLP-1 / glucagon dual agonist anywhere.)
- Drucker DJ. GLP-1-based therapies for diabetes, obesity and beyond. Nature Reviews Drug Discovery. 2025;24(8):631-650. (Broad class review.)
Track this class
GLP-1 Observer tracks clinical trials, news, and regulatory milestones across the GLP-1 and obesity-drug landscape, updated daily. See trial timelines, date-change alerts, and weekly roll-ups.